

Every now and again, this bad recommendation surfaces. I actually saw this printed in an emergency veterinary book recently which prompted me to finally write this article. It’s time to bust this myth.
I think it was the 2008 SOMA conference and the medic’s were presenting their combat medical vignettes. A medic was presenting his casualty vignette when it started going something like this:
“…so I stuck my finger in the wound, and it…no shit…, it felt like a vagina.”
At which point, the entire audience of about 500 collectively looked at their neighbor and asked “did he actually just say that?”. And then he continued:
“…so I put a tampon in it.”
I’m sure almost everyone that has ever received ‘tactical medical’ training, and many that haven’t, has probably heard this advice in some form. Back in 2000 during my EMT ambulance practicum, noticing there were no big field dressings like the Army issued me, I asked my preceptor ‘if we get a really big bleeder, what do we have to use?’ to which he answered ‘probably the diapers’.
Enter critical thought.
To start with, let’s define exactly what the issue is I’m addressing in plain language. Often, so called “subject matter experts” will give the advice, that to treat massive hemorrhage, tampons, sanitary pads and even diapers are acceptable and effective ‘bandages’. The qualification they give is that they are designed to ‘soak up blood’.
I’ve said it before, and I’ll say it again; if you’re ‘soaking up blood’, you aren’t controlling hemorrhage. You are only keeping the floor clean. When someone asks the question ‘how much blood can this bandage soak up?’, they are completely missing the point, and don’t fully understand hemorrhage control.
Sanitary Pads and Diapers
Let me first address sanitary pads and diapers. These are specifically engineered and manufactured to soak up blood and urine and hold it in ‘keeping you dry’. They rapidly wick fluid away from the surface.
If you consider the way blood clots in a wound, this actually works against what you are trying to accomplish. Effective hemorrhage control is to tightly pack gauze up against the damaged vessel, and inside the wound, and hold it under pressure. Medical gauze is specifically designed for this purpose. It puts a significant amount of ‘surface area’ in the form of the gauze fibers in the area where the blood is leaking out. The (manual) high pressure is to minimize this leaking out by squeezing the damaged blood vessel(s) closed. Blood flow is slowed, and with the clotting factors in the blood activated, it becomes sticky, and hopefully sticks to the gauze fibers and all their surface area. With pressure maintained and minimal movement and disruption, hopefully, eventually a clot will form within the matrix of gauze fibers, over the hole in the damaged vessel(s) that will hold and prevent further hemorrhage.
Place a sanitary pad or diaper on a wound and it doesn’t put surface area in the form of gauze fibers in the wound. Rather, it actually wicks the blood away, almost sucking it out of the wound, leaving no clotting or clotted blood present in the wound to seal it. The blood is wicked into the core and clots inside the pad and away from the damaged vessel where it is actually needed to adhere to, to form the plug. Not the best conditions to promote clotting. So the next time someone tells you to use these devices, please educate them on the difference between their great theory of hemorrhage control, and the reality of physiology, physics and the design of these products.
Tampons
The other adjunct I’ll address is the tampon. The theory is that tampons soak up blood so they should be good for hemorrhage control. After all, that’s what they are designed for isn’t it? They come on a stick that seems like it should fit into a bullet wound track, so why wouldn’t it be effective in a gun shot wound for hemorrhage control.
If you understand ballistics, you know that when tissue is struck with a high velocity projectile, the kinetic energy transfer causes both a permanent and temporary cavity. Those cavities also disrupt tissue planes which creates access to potential spaces for blood to pool in internally, as well as following the permanent wound cavity out the entry and exit wound (if an artery is damaged).
Medical gauze sold for packing wounds is usually around 4 inches x 12 feet (144 inches). And a typical gunshot wound will easily eat that entire roll and possibly then some.
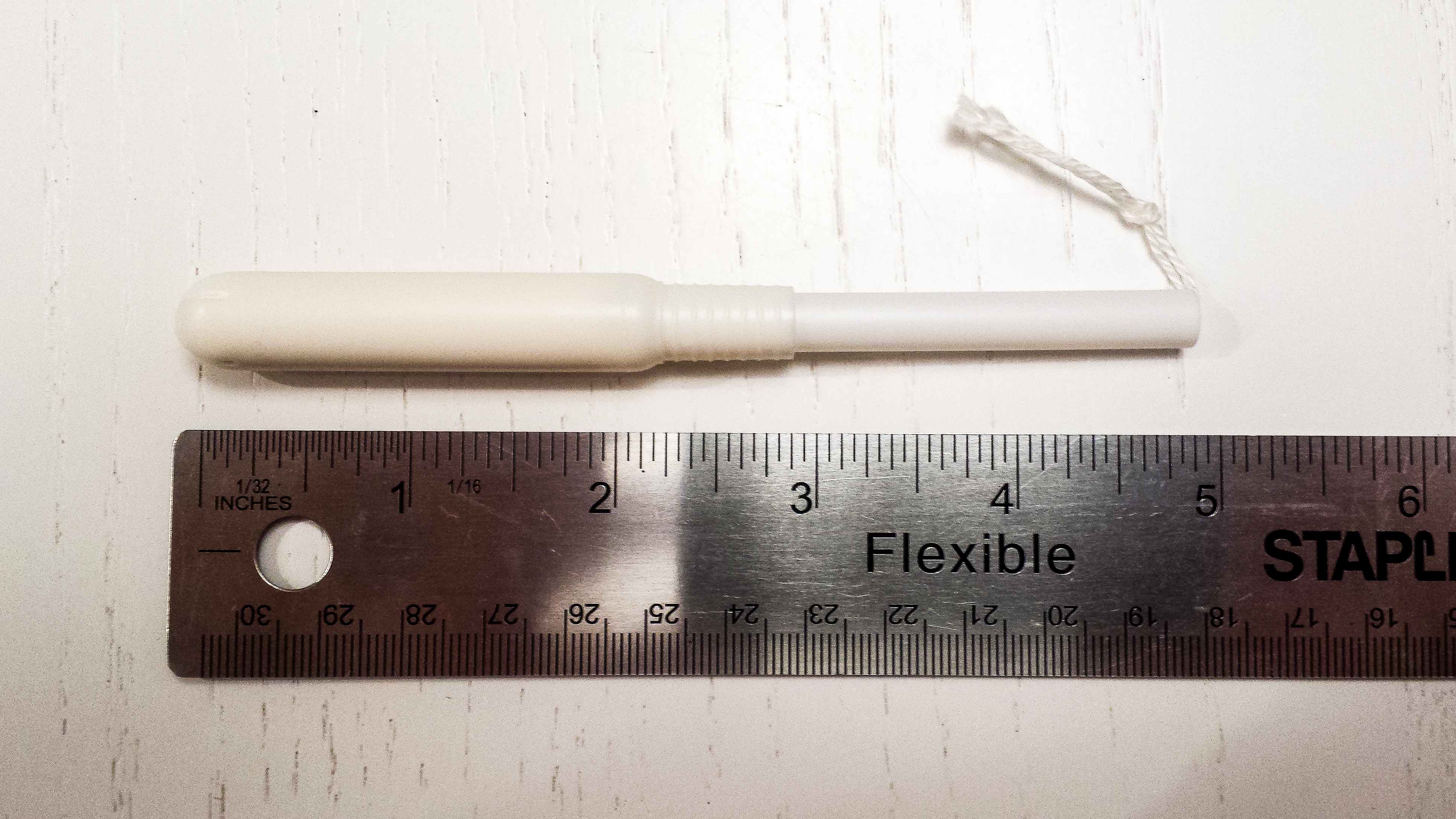
Does anyone know how much gauze is in a tampon? I didn’t, so I opened one up. I needed to soak it in water as it was compressed extremely tight and trying to open it dry, just pulled off little pieces. Little pieces that if they became loose and lost in a wound would be great infection beds.
A tampon is made of two 2 inch x 4 inch pieces of gauze-like material and a little string. And that’s it other than the applicator. Compare that to 12 feet of medical gauze.



 Compare this to the volume that comes in one gauze package.
Compare this to the volume that comes in one gauze package.

A tampon is not designed to stop bleeding. It is not designed to clot blood from a wound. And I absolutely refuse to entertain any jokes whatsoever regarding the natural physiology of the female body. This is serious and respectful business. The bleeding source is not the vagina, but rather from the uterus, and blood flows out through the cervix then the vagina. The tampon is deigned to soak and hold a small amount of blood. The required function is very different. In the presence of a damaged artery, two 2″x4″ pieces of gauze is like throwing a rock at a tank.
Let me leave you with this advice on managing massive traumatic hemorrhage; soaking blood does not equate to stopping bleeding. Once you get past that, you’re on your way to really understanding how clotting, and hemorrhage control works. You need to provide surface area (gauze fibers), including pro-coagulants and or muco-adhesives if available, in and against the actual wound, specifically the damaged vessel that is the source of the bleeding, under pressure, for an adequate duration, so that the minimal amount of blood that does leak out forms a stable clot.
If you need to improvise, a cotton T-shirt can’t be beaten, except by a bamboo T-shirt. Leave the diapers, sanitary pads and tampons alone or else you could be ‘doing more harm’.
January 28, 2015 at 20:19
A very good presentation dispelling a myth I hear constantly. Thank you. This will be referenced many times.
January 28, 2015 at 21:02
well presented. About time somebody put this myth to bed in a sensible manner. I’ve questioned many people about their perceived theory behind using these methods to stop bleeding, to which they had no valid answer. thank you
January 29, 2015 at 07:25
Good start – hopefully somebody at a live tissue lab can apply some solid science to this.
Once upon a time in a world where wound packing wasn’t yet in protocol but gunshot wounds were plentiful, I used many a tampon to fill the permanent cavity left by a bullet. We never did a study and I can’t even anecdotally come to a conclusive answer about whether or not they worked effevtively to stop any hemorrhages, but I know they did help us keep track of how many holes we were dealing with. There is something to be said for that.
And the tampon is easy to control and keep clean in a challenging environment, while I’ve seen roller gauze go rolling down a filthy street a time or two as well.
The surface area argument is good, but I believe the tampon’s absorbency and expansion starts the pressure process inside the wound, no?
Live tissue lab guys get to work and get us an objective and numbers-based answer! My girlfriend wants to know if she can start being suspicious if she finds tampons in my glove compartment.
January 29, 2015 at 08:18
To be sure, a live tissue lab doesn’t constitute “solid science”, but rather only an anecdote. A standard wound model with a control arm and a high number of data points would get you closer, but would still only be Grade 6 evidence, which would actually be good data. I doubt anyone is willing to spend the money on such a study. The article itself could be considered Grade 8 evidence while a handful of casual live tissue uses, while eluding to a bit more information, would actually be rated no different as they are not controlled and could easily and even likely include a degree of bias. It has been done and I am aware of results, but in credible circles they aren’t worth much at all.
Regarding the absorbancy, the amount of outward pressure that a soaked tampon (16 square inches) exerts will not likely overcome systolic blood pressure, and thus do very little to apply pressure to a damaged artery.
January 31, 2015 at 20:31
Every bit of live tissue training I have received has stated do not do this. These are from guys who are all either PJs or 18Ds, and its a myth that needs to die.
February 11, 2015 at 09:46
In 2004 I was told by a Navy Corpsman (FMF) that he was instructed on how to use tampons for hemorrhage control. He even picked up the tampons from the medical command for that purpose. It went against the relatively minimal training I had (essentially pressure and maybe TQ until bleeding stopped), but they way he presented it was professional, and suggested it was probably in a powerpoint somewhere. Thankfully, we never needed it. I’m not defending the use of tampons for anything but their intended purpose, just saying that the information was coming from seemingly credible sources. The military is kind of notorious for picking up and spreading information though.
July 31, 2015 at 08:21
Sorry that I didn’t see this earlier. Way back in the early stages of the Iraq war a lot of FMF Corpsman were taught this, myself included. The big reason was that no one was really willing to spend the money on the new hemorrhage control bandages and devices. It was supposed to be a short term gap measure that has somehow lived on, even to 2010 at Independent Duty Corpsman School. Myself and the few other FMF Corpsman that had a good deal of trauma experienced cringed when we heard this and decided to go over all the other options for hemorrhage control. There are so many products available now, (and many of them have been out there for many years and have good evaluations and tests behind them), that tampons shouldn’t be in anyone’s IFAC/Med kit. Granted, things have gotten a little bit better as far as new gear being issued, for some reason though tampon use is still being taught. It’s better than nothing and I can understand the fiscal issue having to stock some of my junior Corpsman’s bags out of pocket, but there are so many better options out there now.
Former HM1(FMF) Independent Duty Corpsman
October 7, 2016 at 23:41
Strat, I agree, I like this line of explanation and would love to hear more in depth science from a tissue lab. You mentioned that you had used tampons years ago as a gunshot wound pack. Well, years ago tampons were made differently, more of a one piece cotton gauze. Now they use more manufactured synthetic substances, which in my opinion are made to leave particles behind. Not healthy for tissue contact. When discussing this article with my sibling, he mentioned that in a gunshot wound scenario even a modern day tampon might work from a plug/ pressure standpoint if no first aid gauze was available. His argument was, what will kill you faster, not plugging and pressuring the hole or plugging it with something that leaves particles behind?
January 29, 2015 at 08:53
ill admit, I’m not an EMT but do work as a nurse and I keep a trauma bag in my jeep ( Ya never know) I was actually told about this tip/ trick by a firefighter ?? Now that you have dummie proofed it, it all makes perfect sense. All tampons will be becoming out of my trauma bag thanks!!!
January 29, 2015 at 09:52
Years ago when I received my EMT training we were taught to use Tampons on wounds and pads to absorb blood. I know we used many of both, because we did not have funds to buy huge quantities of wound packing. Many squads including mine, were volunteer, funding was beg,borrow & steal and I must add nurses and staff in hospitals. Thank God for these angles. Apparently money is no longer the issue it was, and I am very happy for every one involved. Put the napkins and tampons away folks, the protical has changed.
February 11, 2015 at 09:49
Having bought tampons for women many times over the course of the years, I find it hard to believe that they were actually cheaper than appropriate dressings, when you account for the amount you would have to use of each to make it work. Many departments are penny wise, pound foolish, as they say.
January 29, 2015 at 11:51
I must say you have a great presentation, but your theories are all wrong. If you have a gun shoot wound that is bleeding. Place even gauze on top of the skin does not do much for hemorrhage either. So let me see your point is stopping the bleeding artery, well and absorbent well placed gauze or tampon would remove the clot when it is pulled away. But as long as these material are in place they would start the clot process to slow bleeding. As far as control, that takes a surgeon . So they true treatment is slow the bleeding if it cannot be stopped, and rapid transport to a trauma center. To make my final point, have you ever heard of someone with blood leaking in the abdomen and the surgeon leave it alone, to see if it will clot on its own. I have and yes sometimes it will stop on it own. Of course this is a leak not hemorrhage. However the job in massive trauma is the stabilize as much as possible and get them to the surgeon. It take all of two seconds to insert a tampon into a wound to slow bleeding at the site (does not stop anything internally bleeding). And now concentrate of airway management, IV therapy and all the other stabilization that goes into the total package of proper patient care. So you keep taking your minutes making a fancy dressing while I will be giving my patient total care. Gun shot and fragment wounds need blood transfusions and a surgeon. So to all that might read, slow the bleed and get the patient were they need to be. Chris I do not how long you been doing patient care, but just because you take issue with one of many tools to patient care does not mean that your right in your observations. I have been doing emergency medicine for over 35 years and have never heard a more well presented misleading piece of literature in my life,
January 29, 2015 at 12:14
i do not think we read the same article. At NO point in the article was wound packing ruled out. In fact, wound packing is a critical part of CTOMS TacMed program. The one responsible for the LOWEST DOW rates in Canadian history in Afghanistan.
What I read was to use the appropriate product for the job, NOT improvise with a feminine hygiene product.
There are much improved products for hemorraghe control in the last 35 years. Welcome to the 21 century.
January 29, 2015 at 12:43
While I’m having trouble following your reply, I’ll try to address a few point that you make.
In the field, the issue of removal is of no concern. If you put it in, you leave it in if it’s working. If it’s soaking through, then remove whatever you have packed and start again fresh. The surgeon will remove the packing so who cares if it blows the clot, its not your concern. S/He get’s paid the big bucks to fix it. And you can certainly control hemorrhage without a surgeon, not just slow it down. Your assumption that rapid transport is available for every situation is also a dangerous assumption.
Regarding the comment of an abdominal hemorrhage, and monitoring it without treatment. First, this article is talking about field treatment. Second, you should not be packing abdominal wounds unless you are a surgeon. Third, a surgeon hoping a small mesentery bleed clots itself, and someone in the field hoping a massive femoral artery bleed clots itself are apples and oranges.
If your approach to a femoral artery bleed is to insert a tampon – literally one 4″x4″ piece of gauze, and then go make sure the airway is open, then start an IV on a casualty with an uncontrolled hemorrhage, then you are practicing medicine that is 35 years old and has significantly evolved. You may want to consider some refresher training.
Tampons, sanitary pads and diapers are not, and should not be ‘tools to patient care’. Nowhere on the box does it provide instructions for such use, and none of them hold FDA, CE or Health Canada licensing for such.
I thank you Sir for your comments. I believe you have reinforced my argument.
January 30, 2015 at 08:35
Does no one here use a tourniquet????
January 31, 2015 at 15:41
Tourniquets aren’t the best solution for abdominal wounds…
January 29, 2015 at 15:31
What’s your level of certification?
December 9, 2015 at 07:37
You do realise he was talking about gunshot wounds on the battlefield and about stabilising a wounded soldier to get them to a hospital for a surgeon to then work on them and the misinformation been thought about battlefield management of bleeding and stabilising a gunshot wound.
January 30, 2015 at 10:16
Tampons may not be good for gunshots, but they are awesome for bloody noses.
January 30, 2015 at 11:00
My gods, the derp is strong with many people.
Thanks for the article. This is a sadly under-addressed myth in our community, particularly as we professionals and trainers intersect with lay-persons (students, non-medically trained professionals, etc). Sad that it even has to be addressed, and sad that since it does, more people haven’t. Well done here, will be sharing this (probably often… *sigh* ).
January 30, 2015 at 11:01
Disagree. Exsanguination can only be prevented by arresting blood flow. In a pre-trauma care environment, a tampon will work. Yes, it’s less than ideal and yes, tissue damage may occur…but when minutes count, a tampon can make a difference. -12 years registered RN, 8 years LE Tactical Unit Paramedic.
January 30, 2015 at 13:06
I think you are confusing tamponade (the verb) with tampon ( the scented feminine hygiene product).
January 30, 2015 at 13:48
I get what you’re saying, and for practical purposes, you are right. If someone is injured at home, work, or in a public setting, get them some proper first aid help. This tip is designed for like severe emergency situations. And I have actually seen this work. Some friends and I were camping, he got shot in the leg with an arrow. It was bad. It took us 3 days to get back to our vehicles. The tampon kept him from bleeding out. Once a tampon gets full, it just kind of acts like a cork. A little blood will still leak out, but most of it will stay in there. Like I said, the tampon isn’t for practical first aid, it’s for holy shit that’s a lot of blood and we are days away from a hospital.
January 30, 2015 at 14:00
An arrow and a bullet are very different. ‘Corking’ an arrow wound might work in certain circumstances. It might work if an artery wasnt even hit. It also might work if an artery was hit, and the ‘cork’ effect of the tampon can overcome systolic blood pressure. The wound track is pretty narrow. But, as explained in the article, GSW’s cause a temporary cavity that can peel open tissue planes, making the internal potential space much larger. The amount of blood that has to leak out and tamponade after you ‘cork’ it with a tampon, in order for the hydrostatic pressure of the hematoma to overcome systolic blood pressure of the bleeding vessel is probably going to significant, and not nearly effective.
The article is speaking in broad terms and many people here and on Facebook are trying to find the exceptions and holes and say “it’s great for nose bleeds” and “if it’s all you’ve got then it’s still good”. Yes, if you’re Naked and Afraid, it might be all you’ve got. But usually everyone has a piece of clothing that will probably do a far more effective job in terms of improvisation.
January 30, 2018 at 09:25
Most brodhead on arrows for hunting open a 2″ wound and will go thru if not direct hit on bone.
It’s much more than just a target arrow with a field tip, quarter inch.
Thanks for info you gave.
January 30, 2015 at 16:52
Okay, people… I’ve seen you coming down on both sides of the argument.
For me, it boils down to, “In the presence of a damaged artery, two 2″x4″ pieces of gauze is like throwing a rock at a tank.” Agreed.
What is not stated – and what I feel SHOULD be – is that if you’re not stopping arterial blood flow, a tampon or pad, in the absence of “circumstance-appropriate tools and materials” – is better than nothing at all. It may, depending on circumstances, be better than the suggestion of using a t-shirt.
There’s a lot of back and forth, but nothing, not a damn thing, will suit you better than a decent CPR/BLS course that teaches WHY we want to stop that blood flow.
Once you understand why, the “how” becomes pretty academic by comparison.
This article doesn’t mean “take tampons and pads out of your emergency kit.” It means, “use the right tool for the job, and if you don’t happen to have the right tool, use what is available.”
Looking for one simple, easy rule to follow, simply isn’t viable when you’re talking about a complex and interconnected set of systems.
January 11, 2016 at 11:07
Light at the end of the tunnel.
1) ID the problem …. is it slowly bleeding or is it spurting? TWO very different problems.
2) What do you have with you that best addresses that problem?
3) Do what you can to control the problem and prepare for transport if available.
Pressure is required for arterial bleeding not so much for everything else.
Remember to act in a manner that will calm the injured person so that their blood pressure will not spike any more than it already has.
January 11, 2016 at 11:26
Not all arterial bleeding spurts. Not all arterial bleeding bleeds immediately post injury considering arterial spasm and vasoconstriction from adrenaline. Correct me if I’m wrong, but low blood pressure is something we want to avoid in a hypovolemic patient.
January 30, 2015 at 23:06
Great article and thanks for the info. Quick question I noticed you said “cotton shirt can’t be beat, except for maybe a bamboo shirt.” What properties does bamboo have that would make it better as an improvised wound pack?
January 30, 2015 at 23:49
Of all natural fiber textiles, bamboo has the best hemostatic properties. I don’t know exactly the reason. Though I hesitate to say it because someone will cut a piece off their attic insulation and stick it in their first aid kit beside their tampons, fiberglass is the most hemostatic of man made fibers, and far superior than even bamboo.
January 19, 2017 at 16:21
The idea of raw fiberglass being packed in a wound just sent a cold shiver down my back. That said, it could maybe be a decent fill material inside a more medically apprpriate packaging. Still horrifying.
January 30, 2015 at 23:40
There is some validity to the claims. Historically, Kotex was originally tested and used as a bandage in WW1. Thats where the whole thing originates. Now from everything I’ve ever heard or seen, the tampon works for GSW’s because of its expansion properties which is derived from its high absorption rate. When inside the wound it absorbs and rapidly expands in a small entrance wound providing circumferential pressure. Now its definitely not a cure all… However; I would still use it in the event I had no better supplies or limited time. The Army never sold it as a cure all. Just a time saver or improvisational tool. Military medicine is a whole different beast then civilian. Sometimes you just don’t have the time or supplies
January 31, 2015 at 12:44
So many experts, so little time. 🙂
January 31, 2015 at 19:26
I think the point that many people are missing- is that the article is stating the fallacy of previous teaching (which I heard for years), that tampons are the BEST tool for the job.
They are not, and in fact they never were.
Of course if you have NOTHING else, then use what you can to slow a bleed and allow you to apply pressure, or to pack etc. BUT, if you are doing work in which GSWs are a likely issue- then carry the appropriate gear.
Modern sealed packing gauze and dressings are quite small, and weigh almost nothing. In comparison to the old “tampons are the BEST” strategy- modern dressings are a game changer.
Good stuff Chris.
January 31, 2015 at 23:31
The main concept your forgetting is pressure. A tampon will work just as well as packing gauze if pressure is applied. Chris i dont know where you practice but but if your packing is not workingandits soaking through…. You do not remove it, you add more gauze and continue pressure. By removing it your removing any type of clot that may have started and starting back at square one.
November 8, 2015 at 15:56
Thank you, Roger, for saying that. I’m an EMT-B & we have been taught to not remove dressings that are soaking through, for that very reason – we don’t want to dislodge any clot that may be forming. Pre-hospital care is a different critter indeed…
January 30, 2018 at 09:34
That’s what I hear, keep adding to it.
Never pull out and start again
February 1, 2015 at 02:17
“In the presence of a damaged artery, two 2″x4″ pieces of gauze is like throwing a rock at a tank.”
Although some of your insight is a little off base, the quote above really caught my eye. The artery example is so off topic here. If someone has an arterial wound, my first concern has nothing to do with how I am going to pack it. Stopping blood traveling towards the breakage in priority one. Tourniquet first priority. If wound position does not allow, pressure points are secondary. I would love to be able to go in and clamp them, but fully severed, they retract and that is not always possible, even if they don’t, having enough exposure to perform the task is extremely difficult in a field situation. As far as packing, once its in, it stays in. If you need to add additional packing once you are in a safer situation, that is fine, but you should never remove once in place. If you can slow the bleeding until evacuated to a safer location, inside a medical evacuation vehicle, or at least behind a barricade, then that is a plus. Any particles that might separate from the packing is not the medic’s problem. Once the casualty has been evacuated to a surgeon, they will do what is necessary to remove packing, irrigate the wound, and provide any intervention required to sustain life. I have never used a tampon myself for a medical evac, but I can understand the quick fix until more proper care can be applied.
The plus side of all this, since about 2005, all the soldiers that I was serving with in combat arms were all provided small medical pouches that had a good amount of medical supplies to provide first responder care either on themselves, or a buddy to use the casualties supplies to control bleeding until a medic could get to them. No need to run around with tampons.
February 1, 2015 at 04:09
Why do these debates always end up in dick fencing?
Is it not possible that you are all correct?
Does it not depend on the size of the hole?
If it is a BIG hole then yes a tampon will not provide enough pressure!
If it is a small hole then surely it is the identical to the same amount of gauze packing!
The problem is we all have our own mental picture of the size of the hole.
Just my humble opinion.
February 1, 2015 at 09:32
I understand that this article has probably taken unintentional aim at some ego’s that have recommended this in the past, and some possibly will continue to recommend it in the future. The first reaction in the 10 steps of evolution to acceptance of a new idea is Indignant Rejection. So I guess it all depend on where you fall on the Dissociation of Innovations Curve as to how fast you move through the steps, or if you even ever will. It’s up to you to critically evaluate the article and decide whether you want to accept it or reject it and continue to believe what you do, or change your position. Hubris runs thick in medicine, particularly pre-hospital medicine. As most should know, the more you know about a topic, the more humble you usually are.
This article was never indented to be a comprehensive hemorrhage control class. Nigel is correct in that everyone has their own mental picture about how big the hole is, whereas the article was written in broader terms. Those who feel the need to let the world know how much they know about hemorrhage control in critique format, only reveal the limitations of their knowledge among other things. And that’s ok. I welcome and appreciate every comment. Without critique, no one would ever question themselves, and improvement wouldn’t happen. The comments are all set for manual approval and I have shared every one of them, regardless if I agree or disagree with the content.
Regarding specifically removing gauze after it’s been packed, in my limited experience with massive hemorrhage, if the packing fails, it is most often because it never reached the damaged vessel to begin with. Removing it doesn’t dislodge any significant clots because none have formed where they need to form yet – hence the packing failing and bleeding continuing. And while it’s not a simple as that, this comment isn’t a comprehensive hemorrhage control class either. But what do I know? I’m just a blogger with an opinion and this is a blog not a peer reviewed published study. I’ll be the first to recognize that. Please keep the comments coming.
PS: pressure is covered in the article.
February 1, 2015 at 12:26
“These are specifically engineered and manufactured to soak up blood…” This is a GREAT point. Both my lecture and first aid pack are going to change.
j
February 1, 2015 at 19:30
Good lord, there’s a lot of butt-hurt here. Chris, the reason why fiberglass is the most effective is, ironically, because of something called the “Glass Effect”. Look it up, it’s fascinating reading. Thank you for doing this article.
Also, for those that – rightly so – bring up wound-packing, I would argue that you can absolutely use a t-shirt to pack a wound. Far better than you can accomplish with a tampon. The ONLY appropriate use of a tampon in trauma is soaked in Afrin and jammed up the nares to staunch epistaxis. That’s it. If you use it for any serious, life-threatening trauma other than that, you are, as a point of fact, wrong.
February 14, 2015 at 02:14
I am not agreeing or disagreeing with the use of tampons or sanitary pads, but two points that I would like to add are: they are cleaner than my tshirt and when I first started using feminine hygene products, they were much different than they are now. Especially pads, they were much less absorbent. Now they have different materials that allow them to soak up a LOT of blood. It is possible that the recommendations were made with much different products in mind.
February 15, 2015 at 02:25
I read your article and you are completely correct. I am a CPT and in the 2 years of schooling clotting was extensively discussed. Gauze and pressure should only be used to control bleeding and hemorrhaging. The body uses the gauze and it’s natural clotter called Fibrinogen to close a bleed source. I went to school in 1985 and have worked in labs, hospitals and Dr.s office since and this is the first time I have ever heard of using diapers, pads or tampons. I was actually really surprised not only as a woman, but as someone whom has worked with blood and wounds for years. Thank you for your time and great proven advice.
February 22, 2015 at 13:26
It has been tried in live tissue and failed. Like the article points out, goal is to pack tightly and stop blood flow from vessel, not soak up and wick away.
February 28, 2015 at 18:57
Quite frankly, I’m amazed at how many still not only believe in this practice but espouse its use. Give yer heads a shake. Back in the dinosaur days we were taught this tripe. We believed it, ’cause our instructors believed. Well you old naysayers, guess what? The dinosaurs are dead.
Chris and the CTOMS crew, Bravo Zulu and keep it up.
July 27, 2015 at 04:58
I’d like to read more from the live tissue labs if you have the source.
July 27, 2015 at 07:25
What a great article; well done! Coincidently, a co-worker mentioned the use of tampons for hemorrhage control just the other day. Having never heard of this or anything like it, I thought this was an old practice and otherwise long forgotten. The risk of infection caused by microfilaments left behind seems reason enough not to employee this as a means of hemorrhage control.
August 20, 2015 at 09:20
Stick to using tampons for water collection in remote locations 😉
December 27, 2015 at 17:46
Stop. Just stop.
Using absolutes like “don’t ever use tampons or maxipads” is going to cause far more harm than not.
The medically and intellectually appropriate comment here is that there are better alternatives to tampons and maxipads, and that if you have the option to prepare in advance, there are FAR better alternatives. That said, if your options are tampons/maxipads, or NOTHING? Use them.
Re: “wicking away”… diapers? Yup, that’s what they’re designed to do. Tampons/Maxipads? Not so much.
For anyone who’s jumping on the OP’s bandwagon, for god’s sake, get to a damn CPR/BLS class and talk to someone, interactively, about this topic. If you’re using your head about the issue, then you’ll quickly realize that yes, while there are times when a tampon/maxipad is a bad idea, there are also times when it’s a GOOD idea.
After all, hemmorage control isn’t the ONLY circumstance where the tampon/maxipad gets used.. wound control is as, if not more, prevalent than open hemmoraghing.
Gotta use your brain, people.
January 11, 2016 at 11:27
What’s wound control?
February 27, 2016 at 13:55
take into account the absorbancy of the tampon and think for a second of what it is made out of…. compressed cotton fibers… now take that roll of gauze and think about what it is made out of… spun cotton fibers.. now compress that roll of gauze to the exacting density of the tampon… the fiber count is significantly higher in the tampon vs. the gauze… now consider the act of packing gauze into the hole and how much is needed to absorb the blood and hold it there until it forms a clot… then consider how many tampons are needed to accomplish the same goal while holding the same volume of blood in the same spot until the clot forms on the outer surface of the tampon once its max absorbency has been reached… the logic in your article while an interesting thought simply doesnt work nor do the numbers lie… your right in that a tampon is designed to and does absorb blood but the key is slowing it down to activate the natural clotting response … furthermore a maxi pad can accomplish the same goal for lacerations and is relatively easy to remove if used in conjunction with gauze pads and bound in place much like a combat dressing (same principle in fact) if one is to look at the feminine pads of yesteryear then one would see the similarities in both size /composition/and absorbency as a combat field dressing of today just lacking the binding fabric… all this from my former infantry C/O oregon national guard and corroborated by our medic… so … thats that… hope this helps anyone reading the comments and thanks for listeing to my two cents thus far! keep on keepin on
February 27, 2016 at 22:34
talon;
My first recommendation is that if you want to establish credibility from an academic perspective, you should pay attention to detail regarding simple things like capitalization, punctuation, sentence structure, etc.
My second recommendation is that regurgitating a part time infantry officer’s opinion of hemorrhage control as the final gospel may mean you didn’t shoulder check prior to swerving outside of your lane.
By your explanation, you clearly do not understand, nor have experience with hemorrhage control.
Did I just take the troll bait?
March 25, 2016 at 23:33
So much for the “experts.” Good to know. Thank you.
September 17, 2016 at 19:47
Excellent post. I would also like to add that the bleeding that happens during the menses is different from the hemorrhaging that comes from a wound. Menstrual blood doesn’t come from a wound, but from the perfectly normal and natural shedding of the uterine lining when the ovum reaches the uterus in an unfertilized state.
November 28, 2016 at 03:16
I was told that tampons were great for gunshotwounds by my father, who served 25 years in the army.
But hearing this from a medic truly makes me believe my dad was only hear saying.
But he was a officer in the Jag core, so that probably says a lot.